
Cancer immunotherapy has transformed the treatment landscape of oncology by shifting the therapeutic paradigm from direct tumor targeting to modulation of the host immune system. As summarized in the review by Arifa Aman et al., “The Broad Spectrum of Cancer and Immunotherapy: Achievements and Limitations,” modern immunotherapy can be broadly divided into three major strategies: immune checkpoint blockade, adoptive cell therapy, and cancer vaccines.
While these approaches have demonstrated unprecedented clinical success, particularly in melanoma, lung cancer, and hematologic malignancies, their effectiveness remains heterogeneous, and significant biological and clinical challenges persist.
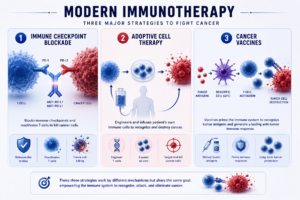
Immune checkpoint inhibitors (ICIs) represent the most widely used and clinically validated form of immunotherapy. By blocking inhibitory pathways such as PD-1/PD-L1 and CTLA-4, these agents restore T-cell–mediated antitumor immunity.
Clinically, drugs such as:
•Pembrolizumab,
•Nivolumab,
•Ipilimumab,
have demonstrated durable responses across multiple tumor types.
However, the limitations of checkpoint blockade are clearly illustrated by clinical trial data. In the CheckMate 650 trial, which evaluated nivolumab plus ipilimumab in metastatic castration-resistant prostate cancer, the objective response rate was 25% in chemotherapy-naïve patients and 10% in previously treated patients, highlighting modest efficacy in this tumor type. Importantly, treatment-related grade ≥3 toxicities occurred in 42–53% of patients, demonstrating that increased immune activation is closely linked to increased toxicity.
This duality reflects a central principle of immunotherapy:
The same immune activation responsible for tumor control can also drive toxicity and limit tolerability.